
During the first peak of the COVID-19 pandemic, nursing homes were dying at a scale that shocked even people who had spent careers studying long-term care. The virus raced through facilities with terrifying speed. Residents shared rooms, shared bathrooms, shared air in long institutional corridors that connected dozens of people in close quarters. Infection control in a building designed to move staff efficiently between large numbers of residents was, in practice, nearly impossible.
Except in some places it didn't happen that way.
A small number of nursing homes — unconventional ones, built on an entirely different model — reported COVID-19 mortality rates that were not merely lower than the national average. They were zero. Not lower. Zero.
In a peer-reviewed study of New York state nursing homes during 2020, Green House facilities reported COVID-19 case rates that were roughly half those of traditional facilities. Zimmerman and colleagues, in a 2021 study published in JAMDA, found that COVID mortality per 100 positive residents was zero in Green House homes, compared to 10 in small traditional nursing homes and 12.5 in large ones. The difference was not explained by resident health status. Green House residents were, on average, older and sicker than residents in the comparison facilities. The difference was explained by the design.
This is worth sitting with. We had, during one of the most catastrophic events in modern nursing home history, a naturally occurring experiment. Facilities built on a fundamentally different model — smaller, more residential, with private rooms, different staffing structures, and a different philosophy of care — performed dramatically better when the most acute test of facility design arrived. And the lesson has not been learned at scale. Less than 2% of the nation's skilled nursing facilities use this model.
What the traditional model actually is, and where it came from
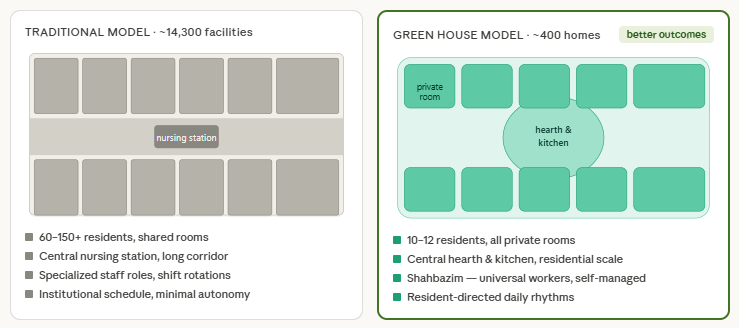
The typical American nursing home looks the way it does because of a 1954 federal law. The Hill-Burton Act, which had previously funded hospital construction, was extended to include nursing facilities. The funding came with design standards — and those standards were derived from hospital architecture. Long double-loaded corridors. Shared rooms. A central nursing station positioned to allow efficient visual and physical access to as many patients as possible. Institutional finishes and institutional scale.
The logic was the logic of efficient hospital care: concentrate clinical resources, minimize staff travel distances, manage a high volume of patients from a centralized point. It was a reasonable logic for a hospital. It is a deeply flawed logic for a place where someone is supposed to live out the remainder of their life.
The hospital model assumes the goal is treatment and discharge. Patients are temporary. Their preferences and daily rhythms matter less than clinical efficiency. The physical environment is secondary to clinical function. This made sense when nursing homes were imagined as short-term recovery facilities. It made no sense when it became clear that most nursing home residents are long-stay residents — that the building is, for many of them, their permanent home for the last years or months of their lives.
The institutional design template was locked in early and has proven remarkably resistant to change. Walking into most American nursing homes today is walking into a building that is philosophically, architecturally, and operationally descended from a 70-year-old hospital model — unchanged not because it works well, but because it is what exists, what is financed, and what the regulatory and reimbursement system was built around.
What the Green House model is
In 2003, geriatrician Dr. William Thomas opened the first Green House homes in Tupelo, Mississippi. They looked nothing like a nursing home. That was intentional. Thomas had spent years arguing that the institutional model was not just clinically suboptimal but philosophically wrong — that it treated residents as patients to be managed rather than people to live fully — and the Green House was his attempt to build the alternative from scratch.
A Green House home houses 10 to 12 residents. Every resident has a private bedroom and a private bathroom. The home is organized around a central hearth — a living and dining area with a fireplace, an open kitchen where meals are cooked and the smell of food is part of daily life, a communal table where everyone eats together. There are no long corridors. There is no central nursing station. The building is, in its bones, a house.
The staffing model is equally radical. Green House homes are served by universal workers called Shahbazim — a word derived from Persian, meaning "royal falcon," chosen deliberately to signal that these workers are not at the bottom of a hierarchy but central to it. Shahbazim provide all direct care: they assist with bathing, dressing, and mobility; they cook the meals; they do the laundry; they sit with residents in the evening and know their stories. They work in self-managed teams. There is no traditional nursing hierarchy in which aides are supervised line workers executing tasks assigned by supervisors. The Shahbaz knows the resident, knows the household, and has the authority to make decisions within it.
Clinical care — nursing, therapy, medical oversight — is provided on a consultant model. Nurses visit. Physicians visit. The permanent staff of the home is the Shahbazim team. The clinical professionals support the home; they do not define it.
Residents direct their own daily rhythms. They wake when they want to wake. They eat when they want to eat. They choose what they eat. They decide whether today is a day for going outside, for watching television, for listening to music, or for simply sitting with a cup of coffee and looking out the window. None of these choices require permission. They are not scheduled. They are expressions of continued autonomy in a life that has moved into a new setting.
What the research shows
The Green House model has been studied more systematically than almost any other care innovation in long-term care, largely because the Robert Wood Johnson Foundation funded the THRIVE Research Collaborative — a multi-year, multi-institution study specifically designed to evaluate its outcomes.
The findings were not ambiguous. Residents in Green House homes were 31% less likely to be rehospitalized within 30 days. They were 38% less likely to develop pressure ulcers. They were 45% less likely to require catheterization — a measure that speaks directly to both the quality of daily care and the culture around resident dignity and dignity-preserving alternatives. They were 16% less likely to become fully bedbound over time.
On quality of life, which is harder to measure but arguably more important, Kane and colleagues asked residents to rate 11 domains of their experience. Green House residents rated their quality of life significantly better in 9 of the 11 domains. The differences were not marginal. Residents in Green Houses reported more meaningful relationships with staff, more control over their daily lives, more sense of privacy and dignity, and a deeper sense of being in a home rather than an institution.
Green House homes provide 23 to 31 more minutes of direct care per resident per day than traditional facilities. This is not because they hire more staff in aggregate. It is because the organizational model eliminates the overhead — the time staff spend walking long corridors, waiting at nursing stations, managing institutional paperwork, and navigating a hierarchical system designed for efficient throughput rather than genuine relationship. In a 12-person household where your primary job is to care for these 12 people, the care reaches the people.
The COVID data, described above, is perhaps the most dramatic single demonstration of what the physical design difference produces. Private rooms mean that an infected resident does not share air with a roommate through a night. Small household scale means that an exposure event involves 10 people, not 100. A self-managing team that knows each resident intimately is faster to recognize subtle changes — a slight confusion, a decrease in appetite — that precede a clinical crisis.
Operating costs, for all of this, are comparable to traditional facilities. Medicare savings from reduced hospitalizations — the 31% reduction in readmissions — can more than offset the higher construction costs of residential-scale buildings. The Green House model is not more expensive to operate. It produces better outcomes at similar cost. The barrier to adoption is not economics, at the level of the operating facility.
So why does less than 2% of the industry use it?
This is the question the outcomes data makes urgent. If the model demonstrably works better — if it produces fewer hospitalizations, fewer pressure ulcers, fewer deaths during a pandemic, dramatically better quality of life — why has it reached fewer than 400 homes in 20 years, while more than 14,000 facilities continue operating on the 1954 hospital blueprint?
The answer is the same answer that explains most of what is wrong with American nursing home care: the financial structure of the dominant ownership model is incompatible with this design.
A traditional nursing home — a large institutional building with 100 or more beds — can be subjected to the financial engineering that characterizes private equity ownership of long-term care. You can sell the building to a REIT and lease it back. You can contract management to a related company at an inflated fee. You can supply staffing through a sister agency at a markup. The scale of the building and the regularity of the revenue stream make it an attractive vehicle for the kind of value extraction that PE firms execute.
You cannot do any of that with a 12-person house. There is no REIT market for residential-scale buildings on a nursing home campus. The management fee on a home that serves 12 people is not worth the trouble. The staffing agency arbitrage breaks down in a model where you need a stable, deeply embedded team rather than an interchangeable workforce. The Green House model is, almost by design, incompatible with the financial engineering that has made large-scale institutional care so attractive to extractive capital.
Only 12 states offer any financial incentive for the small-house model through Medicaid rate structures. The federal government has never passed legislation directing construction support or enhanced reimbursement toward residential-scale care. McKnight's Long-Term Care News noted that for-profit operators have been "particularly slow to embrace" the model — a polite way of describing a sector whose financial logic actively discourages the only design that the research most consistently vindicates.
The regulatory framework is a further barrier. Survey processes designed for large institutional facilities require adaptation for residential-scale homes. Building codes in many states were written for institutional construction and create complications for residential designs. These are not insurmountable obstacles, but they add friction that the dominant for-profit model has little incentive to navigate.
What it actually feels like
The clinical outcomes are measurable. What is harder to convey in a research paper — but central to understanding why the model produces those outcomes — is what it is like to exist inside a Green House home versus a traditional nursing home.
In a traditional nursing home, you are woken according to a schedule. Breakfast is served at a fixed time to a large group of residents, many of whom have been awakened specifically to attend it. Meals come from a central kitchen. The food is adequate, institutionally prepared, eaten in a large dining room or in your shared room. The people who care for you change with every shift. The person who helps you dress this morning may never have met you before.
In a Green House home, you wake when you wake. Someone you know — the same person who helped you yesterday and the day before — asks what you want for breakfast and then makes it, in the kitchen you can smell from your room. You eat at a table with 11 people who have become, over time, something like family. If today you want to sit outside, you sit outside. If today you want to stay in your room and listen to music, you stay in your room. No one needs to approve the decision. The day is yours.
The clinical significance of this is not just psychological. Residents who have agency over their daily lives are more physically active. They eat better because food is prepared in response to their preferences and their hunger, not delivered on an institutional schedule. They sleep better because they control their own sleep rhythms. They are less likely to exhibit the behavioral symptoms — agitation, wandering, depression — that in a traditional institutional setting are often managed with antipsychotic medications. The medication use follows from the design.
How to find one
There are currently approximately 382 to 400 Green House homes operating on roughly 81 campuses across 33 to 35 states. About 90% are operated by nonprofit organizations. About 45% accept Medicaid residents, which means access to this model is not limited entirely to private-pay residents, though availability varies significantly by geography.
The Green House Project, the nonprofit organization that supports the model's expansion, maintains a directory of affiliated homes. NursingHomeIQ surfaces facility type information to help families identify whether a nearby facility uses a small-house or residential model. Beyond Green House specifically, a broader category of small-house models — including the Eden Alternative, the Pioneer Network's culture change framework, and other household-model facilities — share many of the same design principles and produce similar patterns in the outcomes data.
When evaluating any facility that claims a person-centered or residential model, the physical design is the most honest signal. A building with long corridors and a central nursing station is an institutional building, whatever the marketing says about its philosophy. A home where staff cook the meals in a kitchen residents can smell, where 10 or 12 people share a living room, where there is no nursing station because the nurses come to the house rather than operating from a command post — that is a different architecture, and it produces a different life.
The question the data raises
More than 1.2 million Americans live in nursing homes at any given time. The evidence that a fundamentally different model produces dramatically better outcomes — 31% fewer hospitalizations, 38% fewer pressure ulcers, zero COVID mortality at the height of a pandemic — has been available for more than 15 years. The model has been studied, validated, and demonstrated at scale. It has not spread, not because it doesn't work, but because the financial structures that dominate the industry have no incentive to build it.
This is worth naming clearly. The gap between what the research says is possible and what the industry delivers is not primarily a gap in knowledge. It is a gap between what a well-designed care environment produces and what a system designed around financial extraction delivers. The Green House model is not a niche innovation. It is what nursing home care could look like — and what nearly everyone who encounters it believes it should look like — if the financial architecture of the industry were organized around the people living in it.
Less than 2% of the industry uses it. The other 98% is running on a 1954 hospital blueprint.
NursingHomeIQ identifies Green House and small-house model facilities in your area. Search any location to see whether a residential-scale alternative exists near you, and compare it against traditional facilities on staffing, inspection history, and ownership structure.