There is a town in western Nebraska called Chappell. Population around 900. It sits in the Panhandle, a stretch of flat, windswept plains where the nearest city of any size is more than an hour's drive in any direction. For decades, Chappell's nursing home was part of the infrastructure of the community — the same way the grain elevator and the hardware store and the school were part of the infrastructure. When an elderly resident needed skilled care, the options were limited but they existed. The facility was there.
It closed.
What happened to Chappell is happening across the rural United States in a pattern so consistent, and accelerating so quickly, that researchers and policy analysts have started using a specific term for the result: nursing home deserts. Counties where the last skilled nursing facility has closed, where the nearest bed requiring a car trip of 25 miles, 50 miles, sometimes more — and where the family members who might otherwise visit every week now visit far less, because the facility that would have been down the road is in another town, another county, sometimes another state.
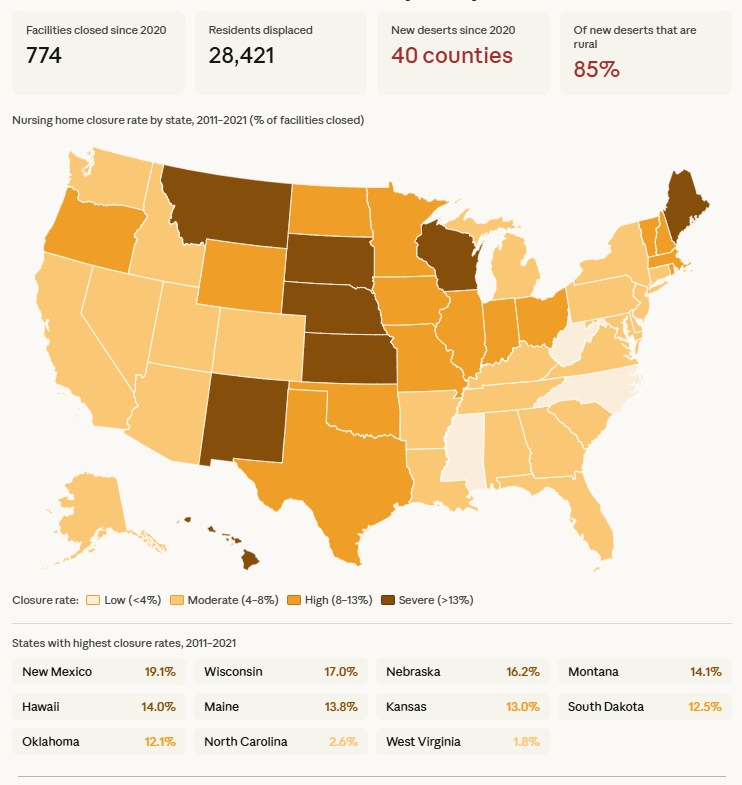
The map above shows the scale of the problem. From 2011 through 2021, the average state lost 8.79% of its nursing facilities — but that average conceals vast geographic variation. The highest closure rates were concentrated in the Midwest, Great Plains, Mountain West, and parts of New England, with New Mexico losing 19% of its facilities, Wisconsin 17%, and Nebraska more than 16%. PubMed Central The lowest rates were in the Mid-Atlantic and parts of the Southeast — states where urban density, stronger Medicaid rates, and larger facility sizes created more financial resilience.
Since 2020, the pace has accelerated.
What "nursing home desert" actually means
Since February 2020, 40 additional counties became nursing home deserts — places where no skilled nursing facilities exist to serve their aging populations. Thirty-four of those counties, or 85%, are in rural communities. American Health Care Association That concentration is not an accident. It reflects a structural reality: the economics of running a skilled nursing facility are difficult under any conditions, and they are most difficult in precisely the places where the need is proportionally greatest.
A nursing home desert is not simply a county that has lost a facility. It is a county where a family facing a care decision for a parent or spouse has no local option — where the choice is not between a good facility and a mediocre one nearby, but between an unfamiliar facility hours away and informal care arrangements the family may not be equipped to provide.
Rural ZIP codes experiencing nursing home closures face average distances of 6.4 miles to the nearest post-acute care provider, compared to under 1 mile in urban areas, with some rural communities having no provider within 25 miles. Wiley Online Library Those distances collapse the informal support systems that make nursing home placement manageable. The spouse who visits every evening. The daughter who stops by on her lunch break. The pastor who comes weekly. Add 40 miles of highway and those visits become monthly at best.
The collapse in new openings
The trend of closures has created nursing home deserts across the country, while simultaneously the rate of new facility openings has nearly stopped. In 2024, only seven new facilities opened nationally, compared to 37 in 2023, 55 in 2022, 71 in 2021, and 73 in 2020. Becker's Hospital Review That is a 90% decline in new openings in four years — and even at 2020 rates, new openings were never keeping pace with closures.
New facilities, when they do open, do not fill the gap left by closed ones. They open in suburban and urban markets where the economics are favorable — where Medicare short-stay rehabilitation patients provide a revenue cushion, where private-pay assisted living is an option, where the labor pool is large enough to staff adequately. They do not open in Chappell, Nebraska, or Dighton, Kansas, or the other rural communities whose last nursing home has gone dark.
Since 2020, there are 62,567 fewer nursing home beds in the United States than there were at the beginning of that year. McKnight's Those beds are not evenly distributed in their absence. The geographic pattern of loss is concentrated exactly where the alternatives are fewest.
Why the economics break down in rural areas specifically
The root cause of rural nursing home closures is not a single problem. It is a convergence of structural disadvantages that each amplify the others.
Medicaid is the foundation. Rural nursing homes serve higher proportions of Medicaid residents — long-term care residents who have exhausted their assets and rely on the government program — and lower proportions of the Medicare short-stay rehabilitation patients who generate the highest per-day reimbursements. For states like Iowa, every dollar spent on Medicaid resident care is reimbursed at roughly 80 cents by the program. In Nebraska, the Medicaid-to-cost ratio is 0.58 — meaning the facility collects 58 cents for every dollar it spends on Medicaid residents. Skilled Nursing News Urban and suburban facilities survive this subsidy through cross-subsidization: the profitable Medicare short-stay patient finances the money-losing Medicaid long-stay resident. Rural facilities have fewer short-stay patients, which means the cross-subsidy is smaller, which means the Medicaid shortfall is more likely to be fatal.
Workforce is the second structural problem, and in rural areas it interacts with Medicaid in a particularly damaging way. Rural nursing homes face high competition for qualified caregivers, and the inability to pay competitive wages — itself a consequence of inadequate Medicaid reimbursement — drives the workforce shortage that then drives the cost increases that then drive the closure. American Health Care Association When a rural facility loses a certified nursing assistant to a nearby hospital or warehouse distribution center paying two dollars more per hour, it cannot replace that worker from a reserve labor pool. There is no reserve labor pool. The alternative is agency staff — temporary workers from staffing companies who cost 40–60% more per hour than direct employees and who bring none of the institutional knowledge that defines quality care.
Occupancy is the third force. Rural nursing homes tend to be smaller — the national average is 107 beds, but rural facilities often operate at 40–60 beds — and smaller facilities have less financial cushion against occupancy fluctuations. When COVID-19 hit, the national average occupancy rate dropped from 82% pre-pandemic to around 74–75%. McKnight's For a 50-bed rural facility operating at those margins, a drop of 8 occupancy percentage points represents six or seven empty beds — the difference between breaking even and losing money every month.
The cascading consequences when a county loses its last facility
When a rural nursing home closes, the consequences extend in every direction.
For residents, displacement means moving to a facility outside the community — often abruptly, often with limited family input into where they land. Research consistently documents that involuntary relocation is associated with declining health in elderly nursing home residents: increased depression, cognitive decline, and mortality in the period following the move. The disruption of established care relationships, familiar environments, and proximity to family is not a minor inconvenience. For a person with dementia, it can be medically significant.
For families, distance transforms the nature of the caregiving relationship. The family member who was the informal quality overseer — who noticed that Dad seemed dehydrated on Tuesday, who flagged that the aide on the night shift was rough during transfers, who maintained the relationship with the director of nursing that ensured concerns were heard — becomes unable to play that role reliably. Research suggests that family presence is itself a quality driver. Its absence is not neutral.
For the community, nursing home closure is associated with a persistent decline in health sector employment of 3–4% overall, and as much as 7–9% in rural counties. PubMed Central A nursing home that employs 80 people is often among the largest employers in a small rural town. Its closure is not just a healthcare event — it removes jobs, it removes the consumer spending those jobs generate, and it signals to other healthcare providers and employers considering the community that the infrastructure they depend on may not be stable.
For the remaining facilities in the region, the dynamics are complicated. Rural facilities that survive a neighbor's closure may see their own occupancy improve temporarily as displaced residents fill available beds. But they also inherit the operational pressures that drove the closure: the same workforce challenges, the same Medicaid rates, the same demographic trends. The stability is often temporary.
Oklahoma: the shape of an accelerated collapse
Oklahoma lost more than 100 nursing homes between 2000 and 2022 McKnight's — a reduction of roughly one-third of the state's total skilled nursing capacity over two decades. The pace accelerated in the post-pandemic years. Oklahoma's Medicaid reimbursement rates have chronically ranked among the lowest in the country relative to actual care costs. The workforce challenges are acute in a state with large rural populations and limited healthcare labor markets in many counties.
The consequences in Oklahoma are visible in the access data. Counties in the western and panhandle portions of the state — historically agricultural, sparsely populated, and dependent on the nursing home as the only skilled care option — have become deserts as facilities closed and no replacements came. Residents who need skilled nursing care must increasingly travel to larger communities, straining both the facilities receiving them and the families trying to maintain connection.
Oklahoma is not unique. It is the accelerated version of a trajectory that multiple states across the Plains and Mountain West are following at varying speeds.
Nebraska's 15 counties without a single nursing home
Nebraska has lost enough facilities that 15 of its counties now have no nursing home at all. In a state where many counties have populations in the low thousands, spread across hundreds of square miles of farmland and pasture, those 15 counties represent communities where the question of what happens to elderly residents who need skilled care has no local answer.
Nebraska's 16.2% facility closure rate from 2011–2021 was among the three highest in the nation. PubMed Central The combination of an aging rural population, chronically inadequate Medicaid rates — with a Medicaid-to-cost ratio of 0.58, among the worst in the country — and workforce challenges that are severe even by rural standards has made Nebraska a leading indicator of where the rural nursing home system is heading.
The communities most affected are not places that policy discussions tend to center. They are small towns where the nursing home was the community's largest employer, its primary healthcare anchor, and the institution that made it possible for elderly residents to age in the county where they spent their lives. When it closes, those residents do not age in place. They age somewhere else, often far away, often alone.
What demography is about to make worse
The timing of the rural nursing home collapse is particularly consequential because of what is coming demographically. The oldest Baby Boomers turned 78 in 2024. The peak of the cohort — those born between 1955 and 1964 — will reach the age of highest nursing home utilization between 2030 and 2040. The population requiring nursing home and long-term care services is projected to grow 40% by 2030.
That demand surge will arrive in a system that has fewer beds, fewer facilities, and a more geographically concentrated supply than it had a decade ago. In suburban and urban markets, the supply-demand mismatch will likely produce waiting lists and elevated prices. In rural markets, it will produce the worst version of what is already visible in the deserts: communities with genuine need and no infrastructure to meet it.
The Medicaid cuts embedded in the 2025 reconciliation legislation — projected at $911 billion over the next decade — will fall hardest on exactly the facilities and exactly the states already closest to the edge. Rural nursing homes are not the facilities that will survive a further Medicaid underfunding pressure. They are the ones that will close.
What families in affected counties need to know right now
If you are a family in a rural community planning for the future care of an aging parent — or if you are the aging parent doing your own planning — the most important thing this data suggests is that the facility you are considering now may not exist in three years. That is not pessimism. It is the documented trajectory of rural nursing home supply in states across the Plains, Midwest, and Mountain West.
Planning for long-term care in a rural county means asking questions you would not need to ask in a suburban market: Is this facility financially stable? What is its Medicaid census and how does that compare to its reimbursement rate? Has it had ownership changes recently? What does its occupancy trend look like? These are questions a family can ask, and a facility's willingness to answer them candidly tells you something as well.
It also means identifying the facilities in the nearest larger community — not as a failure of planning, but as the realistic contingency that rural geography now requires. The distance may be unavoidable. Knowing the options before a crisis makes the navigation of it less chaotic.
The nursing home desert is not a metaphor. It is a county on a map, an empty building on a main street, and a family making a care decision without the options that families in other ZIP codes take for granted.
NursingHomeIQ shows facility locations and status across every county in the United States. Search your county to see what options remain — and how those facilities compare on the measures that predict quality.