
There is a single metric — one number, available in federal data for every Medicare- and Medicaid-certified nursing home in America — that decades of research have identified as the most consistent predictor of clinical quality in long-term care. It predicts whether your parent will develop a pressure ulcer. It predicts whether a medical problem will be caught early or late. It predicts whether a medication error will be made and whether it will be caught. It predicts rehospitalization rates, infection rates, fall rates with serious injury, mortality, and the probability of serious deficiency citations during independent inspections.
It is not the CMS star rating. It is not the quality measure score. It is not the inspection domain, though that comes close.
It is the number of registered nurse hours provided per resident per day.
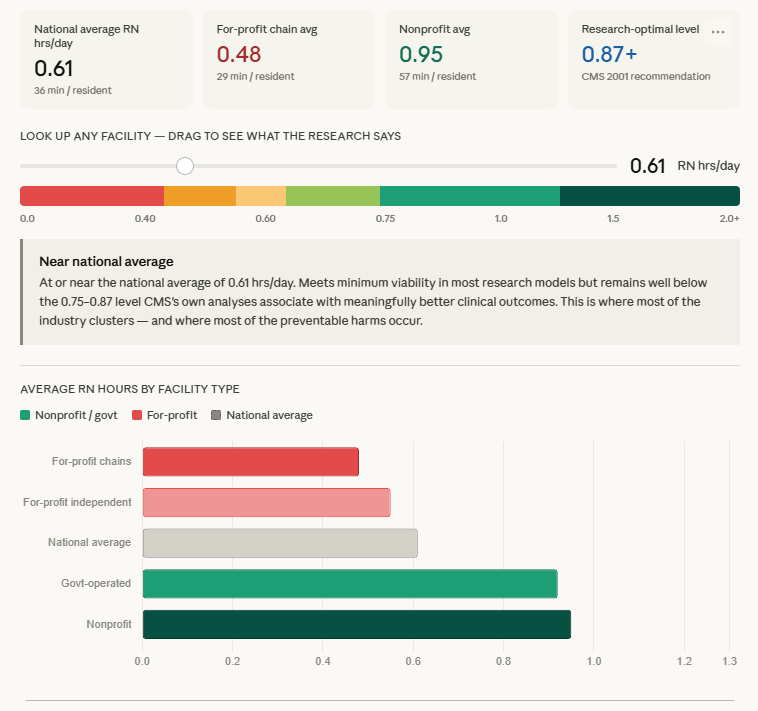
The interactive tool above lets you look up any facility's number and see where it falls on the research-grounded spectrum, from the danger zone to the top tier. The bar chart shows where different ownership types land on average. The national average — 0.61 hours, or 36 minutes of RN time per resident per day — is the context against which every facility's number should be read. That context is important, because the national average is low enough that most of the preventable harms in American nursing home care occur at facilities operating near or at it.
What HPRD means and why it matters
Hours per resident day is a simple calculation: total nursing hours worked divided by total residents. It tells you, on a per-person basis, how much nursing care each resident receives on an average day. CMS reports staffing levels broken out by nursing role — registered nurses, licensed practical nurses, and certified nursing assistants — as well as a total.
The total hours per resident day figure gets cited frequently and is the basis for the staffing star in CMS's Five-Star rating. It is, by itself, a meaningful number. But the research is unambiguous on one point: it is specifically registered nurse hours that drive outcomes. LPN staffing shows no consistent association with safety or quality indicators in systematic reviews. CNA staffing matters too — CNAs deliver the majority of direct hands-on care — but the research finding that distinguishes good facilities from poor ones is RN presence, not total hours.
Why RNs specifically? The answer is in what RNs do that LPNs and CNAs cannot. Registered nurses conduct comprehensive clinical assessments. They identify early warning signs of deterioration — the subtle confusion that precedes sepsis, the slight change in skin color that precedes a pressure ulcer, the pattern of small behaviors that suggests a medication side effect. They make clinical judgments and act on them. They communicate with physicians, manage medication regimens, and initiate the interventions that prevent small problems from becoming large ones.
In a nursing home with 0.40 RN hours per resident day — which is 24 minutes of RN time spread across every resident — the RN is functionally unavailable for anything beyond emergencies. The CNA who notices that a resident seems more confused than usual has no one to escalate to who can clinically assess what that confusion means. The LPN who observes that a wound looks different cannot make the diagnostic judgment about whether it has worsened or infected. The information exists. The clinical interpreter who can act on it is not present.
Where the national average sits — and why it is not good enough
The national average of 0.61 RN hours per resident day is 36 minutes. In practical terms: if a nursing home has 100 residents and provides 0.61 RN HPRD, there are approximately 61 RN hours worked across 24 hours. That translates to fewer than three RN full-time equivalents spread across three shifts on a hundred-person unit.
For context: a 2001 study commissioned by CMS — its own agency — examined staffing levels and clinical outcomes and recommended a minimum of 4.1 total nursing hours per resident day, with an RN component of approximately 0.75 to 0.87 hours. The national average has never reached that recommendation. In 2024, it sits at 0.61 — well below the 0.75 threshold that the agency that funds and regulates nursing homes identified more than two decades ago as the minimum associated with adequate care.
The 2024 Biden-era staffing rule — which required a minimum of 0.55 RN hours per resident day, less than the 2001 recommendation — was the first federal minimum staffing standard in the industry's history. KFF estimated that only 19% of facilities met all staffing components of the rule at the time it was finalized. It was vacated by a federal court in April 2025, delayed by legislation until 2034, and formally repealed by CMS in December 2025. University of Pennsylvania researchers had estimated it would have prevented approximately 13,000 deaths annually. It is no longer in force.
The absence of a federal floor means that a facility providing 0.30 RN hours per resident day — 18 minutes of registered nurse time per resident per day — is operating within the law. Many do.
The ownership gap is really a staffing gap
When researchers document that for-profit nursing homes produce worse outcomes than nonprofits, they are in large part documenting a staffing gap. The most consistent structural difference between for-profit and nonprofit nursing homes is RN investment.
For-profit chains — the segment of the industry with the strongest financial pressure to minimize labor costs — average approximately 0.48 RN hours per resident day. That is 21% below the already-inadequate national average. Nonprofit facilities average approximately 0.95 hours — 56% higher than for-profit chains and well above the 2001 CMS recommendation. Government-operated facilities average around 0.92 hours.
The gap is not primarily explained by differences in resident acuity. Studies that control for resident health status and case mix still find the ownership-staffing relationship. It is a choice — specifically, it is the predictable consequence of an ownership model in which labor is the largest controllable cost and investor returns depend on managing that cost aggressively.
The 10 largest for-profit nursing home chains, which account for a significant share of industry capacity, were documented in a landmark Harrington et al. study to employ 37% fewer RNs than their nonprofit counterparts while receiving more deficiency citations. The causal direction runs from the financial model through the staffing decision to the clinical outcome. Understanding this chain is what makes RN staffing not just a quality metric but a structural signal about the facility's priorities.
The weekend and overnight problem
The RN hours figure reported in CMS data is an average across all days and all shifts. This average obscures a pattern that matters enormously for actual care: the gap between weekday daytime staffing and weekend overnight staffing.
Survey activity — the unannounced annual inspection on which facilities' reputations and ratings depend — occurs overwhelmingly during business hours on weekdays. Facilities that understand this (and they all understand this) have a financial incentive to staff most heavily precisely when the probability of being observed is highest. Weekend overnight shifts, where the probability of inspection is near zero and the marginal cost of additional staff must be justified entirely on clinical grounds, are where staffing cuts are easiest to make and hardest to detect.
Research on temporal staffing variation in nursing homes has documented exactly this pattern: facilities show measurably lower staffing on weekends and overnight, with the gap between best- and worst-staffed shifts being substantially larger than the gap suggested by the daily average. For families, this means that the RN HPRD figure on a facility's CMS profile may not accurately represent what happens during the shift when a parent's breathing changes at 3 a.m. on a Sunday.
The Biden-era staffing rule would have addressed this with a 24/7 RN requirement — ensuring that a registered nurse is present in the building around the clock, not just during business hours. That requirement, along with the rest of the rule, no longer applies.
The practical implication for families: ask specifically. During a facility tour, the question "can you tell me your registered nurse staffing levels for weekday days, weekday nights, and weekends?" is more informative than accepting the overall average. A facility where the answer is confident and specific — and where the differences across shifts are modest — is operating differently than one where the question prompts vagueness or where the ratios between shifts are dramatic.
What the research says about outcomes at specific levels
The interactive spectrum above is built from the research literature, not from arbitrary thresholds. Here is what is behind each zone.
At or below 0.40 RN hours per resident day, multiple studies document significantly elevated mortality and dramatically higher rates of serious deficiency citations. Konetzka and colleagues demonstrated, using instrumental variables to establish causal direction, that the effect of staffing on outcomes is real and that naive estimates likely understate the true impact. Facilities at these levels typically have RN presence only during daytime weekday shifts, with LPNs or CNAs managing all clinical decisions outside those hours.
Between 0.40 and 0.60 — below the national average — the research pattern is consistent: higher rehospitalization rates, more pressure ulcers, worse antipsychotic use rates, and poorer performance on inspection domains. This is not merely correlation: studies using policy discontinuities and ownership changes as natural experiments have demonstrated that reducing RN staffing produces measurable quality deterioration within months.
Between 0.60 and 0.75 — the zone near the national average — facilities are not in crisis, but they are operating below every evidence-based threshold researchers have proposed as adequate. The sector's quality problems are concentrated here, not because this staffing level is catastrophic but because this is where the majority of facilities operate and where most preventable harms occur in aggregate.
Above 0.75, the research literature shifts from documenting harm to documenting benefit. The VA Evidence Synthesis Program's systematic review found moderate-certainty evidence that higher RN staffing is associated with fewer pressure ulcers and possibly associated with fewer infections, lower COVID-19 mortality, and less pain. The evidence becomes stronger as the level increases, with facilities above 1.0 RN HPRD showing outcomes that diverge substantially from the sector average across virtually every measured clinical domain.
How to find and use the number
RN hours per resident day is publicly available in CMS data and displayed in NursingHomeIQ facility profiles. There are two important caveats about interpreting it.
First, the number is a facility-wide average, reported as an average over a quarter. As discussed above, this masks shift-level variation. A facility that reports 0.78 RN HPRD could be providing 1.2 hours during weekday days and 0.30 hours on weekend nights. The aggregate number is informative but not complete.
Second, CMS now reports staffing data from the Payroll-Based Journal — actual payroll records rather than self-reported estimates. This is a significant improvement over the pre-2016 system in which facilities simply submitted whatever numbers they chose. PBJ data is more reliable, though not immune to gaming: some facilities have been documented using creative payroll practices to inflate reported hours. On-call staff who are never physically present in the building, administrative RNs counted toward direct care hours, and contract nurses split across multiple facilities have all appeared in investigations of PBJ data anomalies.
The right way to use RN HPRD is as a primary signal interpreted in context. A facility with 0.45 RN hours per resident day is telling you something about its priorities regardless of what the overall star rating says. A facility with 0.95 RN hours per resident day, combined with a stable nonprofit ownership structure and strong inspection record, has demonstrated a sustained commitment to clinical care investment that is the most reliable predictor of what your parent will actually experience.
The number is not perfect. No single number is perfect. But in a field full of gamed metrics, inflated self-reports, and composite ratings that obscure more than they reveal, registered nurse hours per resident day is the metric that the research has validated most consistently, across the most studies, over the longest period. It is the number that most reliably distinguishes facilities that care about clinical quality from those that have learned to look like they do.
At 36 minutes of RN time per resident per day, the national average is telling you something, too. It is telling you that the industry as a whole has decided that this is enough. The research says otherwise — has said otherwise since 2001, when CMS commissioned the study that established the threshold and then never enforced it.
Knowing what a facility's number actually is, and knowing where it sits relative to both the national average and the research evidence, is not a complete picture. But it is the most important single piece of information available to a family trying to make the most consequential care decision of their lives.
Every NursingHomeIQ facility profile shows registered nurse hours per resident day alongside total nursing hours, staffing star rating, and ownership type — so you can read the signal that the research most consistently validates, not just the composite CMS provides.