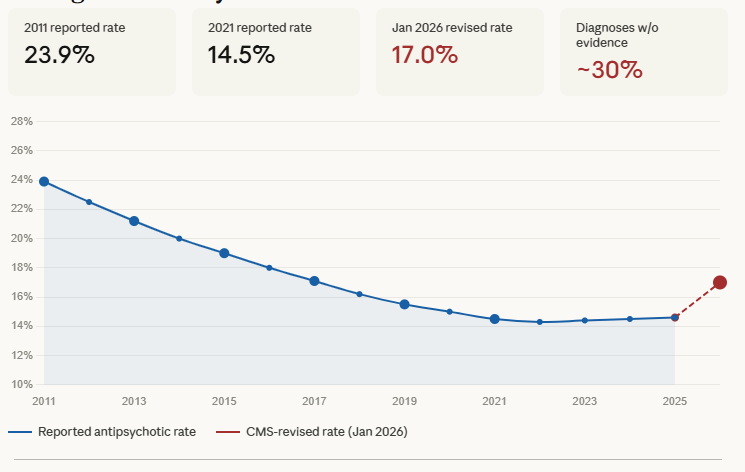
For more than a decade, the federal government has been tracking how often nursing home residents are given antipsychotic medications. The headline story looked like progress: the national rate fell from 23.9% in 2011 to 14.5% by 2021 — a 40% reduction driven by the National Partnership to Improve Dementia Care, a CMS-led campaign that publicly named and shamed high-prescribing facilities.
Then, in January 2026, CMS changed how it measured the number. The rate immediately jumped to 17%.
That jump wasn't a sudden surge in prescribing. It was the measurement catching up with reality. And understanding why tells you something important about how to evaluate any nursing home's reported quality data — including this one.
What antipsychotics actually do to elderly people with dementia
Antipsychotic medications were developed to treat psychotic disorders like schizophrenia and bipolar disorder. In nursing homes, they are frequently used for a different purpose: to calm agitated, wandering, or difficult-to-manage residents with dementia.
The clinical term for this is "off-label use." The FDA's term is more direct: it issued a black box warning in 2005 stating that antipsychotics are associated with a significantly increased risk of death in elderly patients with dementia — roughly 1.6 to 1.7 times the mortality risk of patients not given these drugs.
The harm extends well beyond mortality. Antipsychotics cause sedation — residents who were mobile become less so, which increases falls and hip fractures. They accelerate cognitive decline in dementia patients, which means the disease progresses faster. They increase stroke risk. They blunt emotional responsiveness. A resident who was anxious and difficult at 9 a.m. may be sitting quietly and staring at the ceiling by 10 a.m. — which from a nursing home management perspective can look like success, but from a quality-of-life perspective looks like something else entirely.
Advocates and researchers have a phrase for this: chemical restraint. Physical restraints — tying someone to a bed or chair — declined from roughly 19% of nursing home residents in 1985 to under 1% by 2015, driven by the 1987 federal reforms that prohibited their use except in specific clinical circumstances. But the underlying pressure that led to physical restraints — too few staff, too many residents with complex behavioral needs — didn't disappear. It found a pharmacological outlet.
The exemption that changed everything
When CMS began publicly reporting antipsychotic use rates in 2011, it built in what seemed like a sensible clinical exception: residents with a documented diagnosis of schizophrenia, Tourette's syndrome, or Huntington's disease were exempt from the metric, because those conditions legitimately require antipsychotic treatment.
What CMS did not anticipate — or perhaps did not adequately account for — was that nursing facilities are rational actors operating under financial pressure. A metric that measures something and attaches public consequences to it will be gamed. It is almost always gamed. And in this case, the exemption created an obvious path.
If your antipsychotic rate is too high, and residents with schizophrenia are exempt, the solution writes itself: document more schizophrenia.
After CMS introduced the public reporting measure, schizophrenia diagnoses in nursing homes nearly doubled. The prevalence of schizophrenia in the general elderly population is approximately 0.5–1%. In nursing homes under public reporting, it became dramatically higher.
The Department of Health and Human Services Office of Inspector General investigated and found that approximately 30% of nursing home residents with a documented schizophrenia diagnosis had no supporting evidence of that diagnosis anywhere in their Medicare claims history — no prior psychiatric care, no prior diagnosis, no documented treatment history before their nursing home admission. The diagnosis appeared, in many cases, at or after admission, in facilities with high antipsychotic prescribing rates.
This is the mechanism behind the "improvement" that the national data showed over a decade. Some of the rate reduction was real — facilities genuinely reduced unnecessary prescribing, often through better dementia care training and person-centered approaches that address the behavioral triggers driving agitation. That progress is meaningful and should be acknowledged. But a substantial portion of the measured improvement was a documentation artifact. The drugs didn't go away. The diagnoses changed.
What January 2026 revealed
In January 2026, CMS introduced a revised claims-based measurement methodology designed to close the schizophrenia exemption loophole. Rather than relying solely on nursing home self-reports of resident diagnoses, the revised measure cross-references Medicare claims data to verify whether exempted diagnoses have clinical support.
When the new measure went live, the national antipsychotic rate jumped from approximately 14.5% to 16.98% — a nearly 2.5 percentage point increase that appeared overnight, with no change in actual prescribing. It was the gap between what facilities had been reporting and what was actually happening, suddenly visible.
That gap represents hundreds of thousands of nursing home residents receiving a medication with a black box mortality warning, whose use was being underreported in the quality data families use to evaluate facilities.
Who prescribes most
Antipsychotic use is not evenly distributed. The research shows clear patterns by ownership type and structure.
The landmark Gupta et al. study found that private equity ownership of nursing homes was associated with approximately a 50% increase in antipsychotic drug use. The mechanism aligns with everything else known about PE ownership: lower staffing means less capacity to manage behavioral symptoms through direct care and attention, and antipsychotics become the cost-efficient substitute. A pharmacological intervention that can be administered in seconds replaces an hour of skilled nursing engagement with an agitated resident.
Facilities with lower registered nurse staffing — below 0.5 RN hours per resident per day — show consistently higher antipsychotic rates. This is not coincidental. RNs are the clinical decision-makers responsible for medication management and for escalating to physicians or psychiatrists when behavioral interventions aren't working. When RNs are scarce, the path of least resistance runs through the medication administration record.
Chain-affiliated for-profit facilities consistently report higher antipsychotic rates than independent or nonprofit facilities, even after controlling for resident acuity. Large chains, particularly those with investor pressure on operating margins, have the strongest incentive to maintain the documentation practices that artificially depress reported rates.
What this means for families evaluating a facility
The antipsychotic rate listed on a facility's CMS profile is still worth looking at — it's not meaningless. A very high rate is a genuine red flag. But a low rate no longer means what it once appeared to mean, and a middling rate may represent anything from exemplary dementia care to systematic exemption documentation.
What to look for instead, or alongside, the reported rate:
First, ask directly. When touring a facility, ask: "What is your approach when a resident with dementia becomes agitated?" The answer tells you more than any number. Facilities with genuine person-centered dementia care will describe specific non-pharmacological protocols — redirection, environmental adjustment, activity engagement, identifying and addressing the underlying trigger. Facilities that rely primarily on medication management will often answer vaguely or describe the prescribing physician's role without mentioning behavioral care.
Second, look at RN staffing hours per resident day. The research connection between low RN staffing and high antipsychotic use is robust. If a facility's RN hours are below 0.5 per resident day, the likelihood of adequate behavioral care is low and the likelihood of chemical management is high.
Third, look at the facility's staffing stability. Antipsychotic use correlates with staff turnover. A CNA who has known a resident for two years understands their behavioral patterns, knows their triggers, knows their routines. A CNA who started last week does not — and is far more likely to respond to agitation with an incident report that escalates to a prescription rather than the kind of individualized de-escalation that comes from genuine familiarity.
Fourth, look at the gap between the facility's self-reported quality measures and its inspection history. Facilities that are gaming antipsychotic reporting are often gaming other quality metrics as well. A large gap between stellar self-reported scores and poor inspection results is a coherent pattern, not a coincidence.
What the history tells us
The story of antipsychotic gaming in nursing homes follows a pattern that appears across virtually every quality measure CMS has introduced: measure something publicly, create pressure to reduce it, and watch rational actors find ways to reduce the measurement without necessarily reducing the underlying problem.
This is not unique to nursing homes, and it is not an argument against measurement. Public reporting has produced real improvements. The national reduction in physical restraint use, driven by OBRA '87 and subsequent enforcement, is a genuine success story. Pressure ulcer rates have declined. Re-hospitalization rates have improved in some settings.
But it is an argument for sophistication in how families use reported data — and for platforms like NursingHomeIQ to go beyond presenting the numbers at face value. The antipsychotic rate is a case study in why a single reported metric, evaluated in isolation, can actively mislead the family trying to make the most important care decision of their lives.
The January 2026 rate revision is, in a narrow sense, good news: CMS is trying to make the measurement more accurate. The fact that the rate jumped 2.5 points the moment better methodology was applied tells you how far the gap had grown. It also tells you that the gap closed overnight — the drugs were always being given. Only the accounting changed.
NursingHomeIQ displays antipsychotic rates alongside RN staffing hours and staff turnover data, because no single number tells the full story. Search for facilities in your area to see how they compare across all three.